
The Blackfoot Valley's News Source Since 1980
The Blackfoot Valley's News Source Since 1980
Three-year-old Addy Trevino was diagnosed with and inoperable brain tumor last June. Cells from her biopsy prior to radiation and chemotherapy were donated to research. Addy's cells now make up the first working models of lab-grown DIPG tumors in the world. (Photo provided)
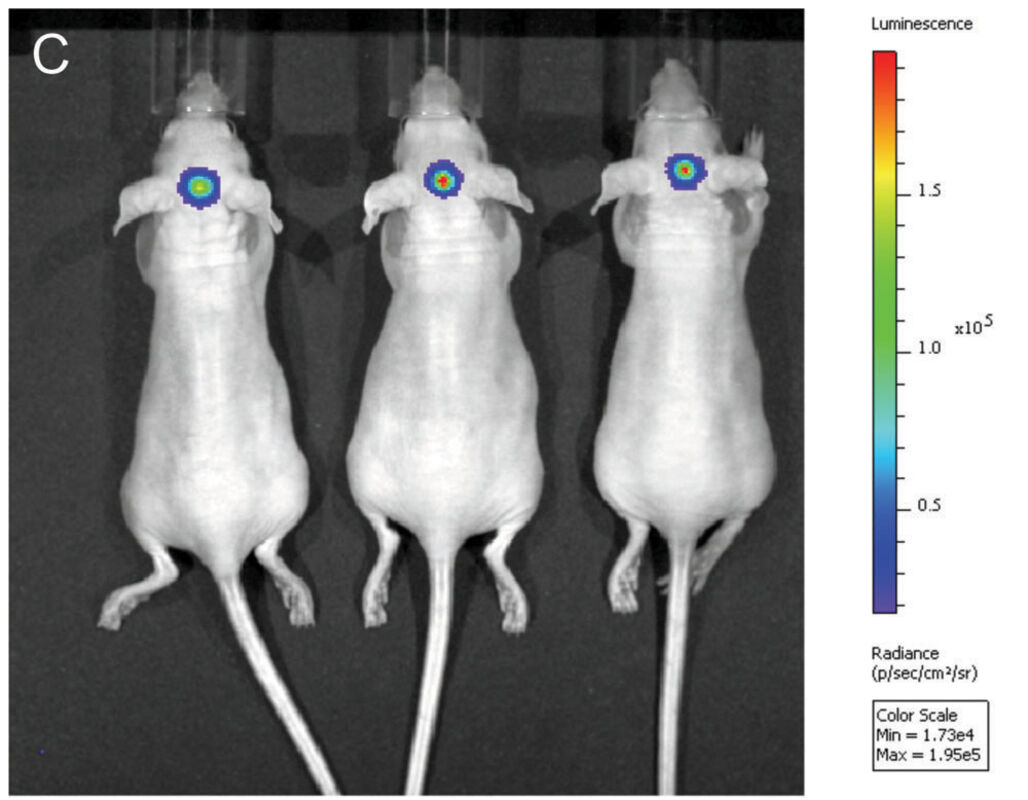
Nude mice after being implanted with mCherry and Addy's DIPG cells. The bioluminescent signal shows DIPG tumor growing and ready for testing
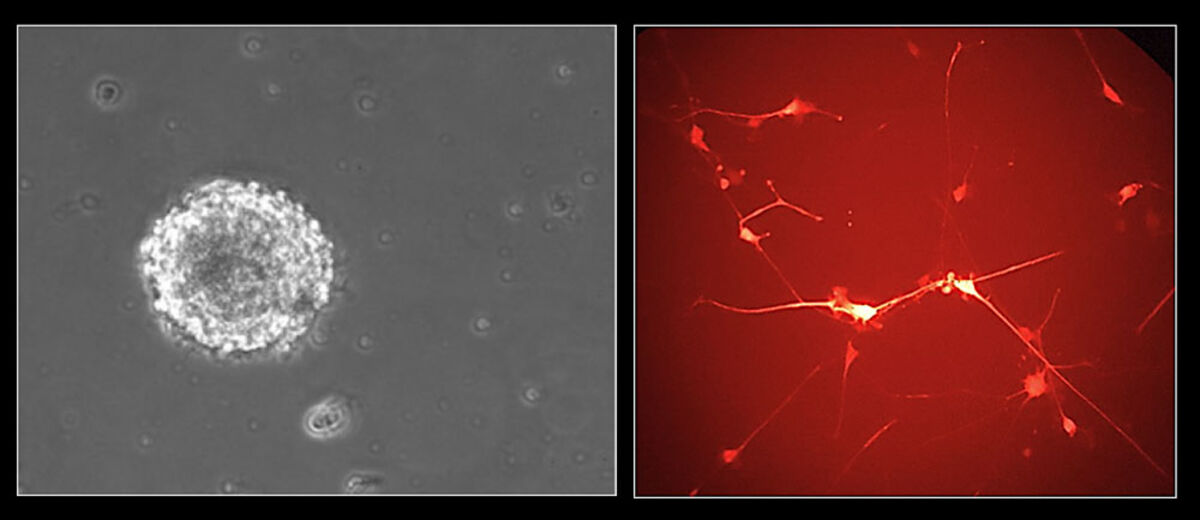
The left slide shows Addy's DIPG cells forming a neurosphere while growing in a media suspension in the Jim Olson's Lab at the Fred Hutchinson Cancer Research Center. The right slide shows Addy's DIPG cells spreading out on laminin after a CMV-mCherry infection to make them bioluminescent (red).
Addy Trevino with her older sister Miya at their home in Seeley Lake. (Photo provided)
SEATTLE - "I had never, at any point in my medical training, sat in a room where at the same time you tell a patient they have a diagnosis, you also tell them they will definitively die from that diagnosis."
This was Dr. Nicholas Vitanza's memory of meeting his first patient with Diffuse Intrinsic Pontine Glioma (DIPG), an inoperable brain tumor found in children. As a pediatric neuro-oncologist at Seattle's Children's Hospital, he has since delivered the same message to many more patients diagnosed with DIPG.
Now, one of his current patients, Addy Trevino from Seeley Lake, Mont., offers new hope to families facing this devastating diagnosis. Treatment naïve cells, removed as part of an optional biopsy, have allowed scientists to replicate Addy's pre-treatment tumor in 20 mice.
"Treatment naïve" is a term for cells that have not already been subjected to, and therefore changed by, radiation or chemotherapy. According to Vitanza, this is the first instance he is aware of in which treatment naïve cells have been grown in a lab. This breakthrough will allow scientists and doctors to learn more about DIPG and ultimately find ways to kill DIPG tumor cells, a mission that Vitanza has made his life goal.
* * * * *
The first paper to report and document DIPG was published in London in 1926. However without an MRI and because children can die within a couple of weeks from worsening neurologic function, Vitanza thinks many more cases may have gone undiagnosed.
Today, around 350 children per year are diagnosed with a DIPG tumor in the United States, most commonly between the age of six and seven. Vitanza has patients who range from age one to 26.
Vitanza explained the name describes the cancer well. The tumor is diffuse and intrinsic to the pons, part of the brainstem that connects the nerves from the brain to the spine. The pons controls eye movement, swallowing, breathing, urination and muscle strength in the extremities.
Vitanza said the problem with DIPG is the genetic mutation takes place in the gene that makes hystones. A hystone is the protein that helps package and organize all the DNA inside cells.
"A lot of the entire genetic code is being processed abnormally," said Vitanza. "We call that an epigenetic problem; it is above the level of one genetic mutation."
Groundbreaking work by Dr. Michelle Monje at Stanford University pioneered the research of taking autopsy specimens of DIPG tumors and growing them in a tissue culture in the lab. Scientists were then able to perform treatment studies that led to incredible breakthroughs in the understanding of the tumor.
Nevertheless Vitanza, who worked with Monje prior to bringing his work to Seattle Children's Hospital and the Fred Hutchinson Cancer Research Center, said, "I think DIPG will continue to be impossible to cure unless we study the cells that are present exactly when a child has the disease. Getting radiation and other treatments causes brand new mutations and tons of changes in the cells."
Vitanza explained that, while most cancer patients have a higher chance of survival if the tumor can be fully removed, because the pons do not have clean borders, the tumor cannot be removed.
"DIPG is one of the very last things in pediatric cancers that is a completely incurable disease," said Vitanza. "From day one we know that there is not going to be anything we can do to save the patient. That is completely unacceptable."
* * * * *
Addy was rushed to Seattle Children's Hospital at the end of June, 2017, after her tumor was discovered on an MRI. She displayed classic symptoms of DIPG and radiation was the recommended treatment option.
"Unfortunately radiation is the only thing that is reliably extending children's lives," said Vitanza. "Without radiation the average overall survival is about five months. With radiation we are able to extend that closer to 11 months. But even with radiation, we are not able to save children with DIPG."
Addy's parents Jen and Treay chose to do the optional biopsy because that allowed them to see if Addy's tumor had any genetic mutations that would qualify her for an open clinical trial. They were asked to sign a waiver agreeing to donate any leftover cells for cell research.
Vitanza explained to the Trevino's that it was unlikely the harvested cells would result in any research that would directly impact Addy. He told them, "The most likely thing is that we will have trouble getting these cells to grow. But if we do get these cells to grow, they could teach us a lot and potentially help children in the future."
"Anyway that she can help, we are all for it," said Jen. Though the biopsy did not qualify Addy for any open studies, Vitanza learned from it so he could suggest potential treatments for it should it start to grow again. In addition to being Addy's clinical doctor, Vitanza spends half of his time designing and performing DIPG research at the Fred Hutchinson Research Center, an associate of Seattle Children's Hospital. Jim Olson runs the lab where Addy's cells are housed. Of the 40 biologists in the lab, 10 work under Vitanza, focused on DIPG research. Scientist Matt Biery and research technician Carrie Myers have worked specifically with Addy's cells.
Half of Addy's cells were put into tissue culture and the other half into four mouse brains. While the cells initially started to grow in the tissue culture, the mouse brains did much better.
The Trevinos didn't learn that the lab was able to grow Addy's cells until late September.
"Nick [Vitanza] said the cells were growing at the lab and that was the first time they were ever able to replicate a treatment naïve tumor," said Jen lighting up with excitement.
"I talked to Jen a lot in the beginning that the most likely thing is that these cells are never going to teach us anything that directly impacts Addy," said Vitanza.
Over the last months, all of the mouse tumors grew and multiple millions of cells have been taken out, regrown and implanted into more mice. The cells were infected with an mCherry virus that makes the tumor glow red under florescent light.
Vitanza said they can put the mice under a little image machine and within a few seconds monitor the tumor growth with this bioluminescence and kind of track the mice and how the tumors are growing.
Olson's lab is working with more than 20 mice growing Addy's cells with opportunities for many more. This not only provides them with a unique ability to study the biology and genetics of DIPG, it allows for clinical tests.
"I would say that this is one of the first in the world, if not the first, working model," said Vitanza. "This will give us a mouse model of the disease that is treatment naïve and that we can start doing studies and testing radiation, drugs and new treatments"
Vitanza said it will provide the foundation for designing more targeted clinical trials for future children.
In the case of Addy, Vitanza said, "the stars aligned." He explained that first a neurosurgen must be able to do the DIPG biopsy. Seattle Children's Hospital is one of a handful of hospitals that does biopsies.
Next, there needs to be a connection to a center that has the required infrastructure to do the laboratory cultures and put the cells directly into mice. Finally, there must be the laboratory system in place to grow the cells.
"Tens of thousands of dollars have been invested into Addy's cells through either research grants or philanthropic donations from local groups," said Vitanza who thanked his funders the Pediatric Brain Tumor Research Fund, The McKenna Claire Foundation and Unravel Pediatric Cancer. "One of the reasons I came to Seattle Children's Hospital was to have a pipeline with this potential. It just turns out that Addy's case has been our first success. But we think that it will be our first success of many."
Vitanza said even this early in the trials, he has started talking with some pharmaceutical companies..
"We are taking drugs that already exist and, with our scientific understanding of DIPG, we can predict what groups of drugs might exist," said Vitanza. He further explained they can test one group of drugs to determine which works best and why. They can also combine multiple drugs. From this, they can develop the clinical trials for patients. Vitanza thinks the most effective clinical trial will be one with multiple drugs.
Seattle Children's Hospital is one of the five largest pediatric brain tumor centers in the country. They work closely with the other centers around the world to run clinical trials.
As Addy's cells are grown and banked, they will be shared with other labs that study DIPG across the country and internationally, as well as collaborate with other labs. Olson's lab will validate all the tumors to ensure they are still identical to Addy's tumor. "The way Nick puts it, Addy has already done so much for the research side of it," said Jen. "Getting the cells to grow was rare and they are specific to just Addy. If they can find something for those cells in the lab that works, it gives us that much more hope that is going to work for her. That was a part of her. If you can cure a part of her, you can cure all of her."
Vitanza said a "really fast" clinical trial with human patients using Addy's cells could show results in just a few years. He is amazed by the emotional fortitude of the Trevino family because of their realization that Addy's brain cells are growing in a lab that could very well outlive her.
"We are so thankful to Addy and her parents for their contribution," said Vitanza. "The donation that they have made is worth more than any amount of money. The research would be impossible without those cells."
While the ability to grow treatment naïve cells is ground breaking towards understanding DIPG, Vitanza said, "I try to remind myself that until we actually help a child, we haven't really made an accomplishment. I try to think that everything we are doing is encouraging but we haven't hit any of the milestones that I want to reach yet. But I think we are making a good start."
From 1960 to today, the survival rate for those diagnosed with leukemia has gone from zero to 94 percent.
"I'm positive that one of these trials will work and a breakthrough will happen," said Vitanza. "Tempering the expectations of families is important [and encouraging them to make the time they have left the happiest possible] but at the same time I'm trying to make sure that one of these days I will take care of a kid that I will say it is the disease that can't be cured and then he/she will be cured. Eventually I'll take care of that kid."
"It's like when they first asked us – anything that Addy can do to help others," said Jen. "Now it is at the point where she IS helping others and she is helping scientists learn about this tumor that has been known about for over 100 years with no results. I'm not saying she is going to be the cure but at least she will have a step in that. If they find a cure for this, even if it is too late for her, at least she did her part."
* * * * *
Addy is now nine months past diagnosis. She finished her radiation this fall and returned to Seeley Lake where the family has been embraced by the community.
"We did radiation and she got better. It was hopeful but they told us it would only help [for about a year]," said Jen. "They walked us out of the hospital and told us to go make some memories. And that's it. It was hard to have any hope at that point."
Their hope returned when the Trevino's learned about Addy's cells growing in the lab. Addy was also doing so well clinically.
"We have absolutely been fortunate because she got back to where she was before she was clinically diagnosed," said Jen. "She was happy, she could play, she was on very, very few medications."
Even with symptoms resurfacing after being home for the past six months, she's happy and "she's still a little monster." She is not in any pain. She is undergoing maintenance chemo every two weeks. The Trevinos continue to research clinical trials.
"It still affects her everyday life," said Jen. "She doesn't have a smile on her face until we reassure her that there is no doctor. That she doesn't have to 'get no pokes.' It's just not fair. I just focus on the innocence of childhood cancer. The [children] never did anything to deserve it."
At Addy's last appointment April 13, the Trevinos learned that the tumor started to grow again. Though smaller than her original tumor, it is still about 10 percent larger than her previous scan. They will be discussing possible options with Vitanza next week.
"She is still a happy three-year-old right now," wrote Jen on Team Addy Boo's Facebook page. Addy Boo is Jen and Treay's nickname for Addy. "From this point forward, her happiness is what we want to focus on. We'll take the next step when we need to."
Jen added, "I want to genuinely thank everyone for your prayers, thoughts, and support. Dr. Nick (Vitanza) has been awesome through this whole thing."
There is a Benefit for Addy Boo scheduled for April 28 from 2-7 p.m. at the Church of the Nazarene, 2339 25th Ave. Missoula on the corner of 26th and South Avenue. Please contact Mona Bennett, 406-239-2970, if you would like to help with the benefit. Everyone is encouraged to attend.
Reprinted with permission.








Reader Comments(0)